Does Entrepreneurship Make a Difference in Health Care? The Case of Private Funded CHSLDs

Viewpoint showing that facilities funded by the public purse but run by entrepreneurs provide a better environment for patients, while costing the government less
What does entrepreneurship contribute to health care? Despite the example of Europe, where companies have long had a large role to play within universal systems, simply posing this question in Canada can elicit strong reactions. And even when European successes are mentioned, other reasons are always suggested to explain their better results. Is it possible to isolate the “entrepreneurship” variable? The example of Quebec’s CHSLDs can help us in this regard.
 Related Content
Related Content
 |
 |
 |
| L’entrepreneuriat fait-il une différence en santé? (Le Soleil, October 3, 2019) | Interview (in French) with Patrick Déry (Politiquement incorrect, Qub Radio, October 3, 2019) | Interview (in French) with Patrick Déry (Mario Dumont, LCN-TV, October 3, 2019)
Interview with Patrick Déry (CTV News Montreal Noon, CFCF-TV, October 3, 2019) |
This Viewpoint was prepared by Patrick Déry, Senior Associate Analyst at the MEI. The MEI’s Health Policy Series aims to examine the extent to which freedom of choice and private initiative lead to improvements in the quality and efficiency of health care services for all patients.
What does entrepreneurship contribute to health care? Despite the example of Europe, where companies have long had a large role to play within universal systems, simply posing this question in Canada can elicit strong reactions. And even when European successes are mentioned, other reasons are always suggested to explain their better results.(1) Is it possible to isolate the “entrepreneurship” variable? The example of Quebec’s CHSLDs can help us in this regard.
Quebec has just over 400 residential and long-term care facilities (“centres d’hébergement de soins longue durée” or CHSLDs).(2) These mainly serve seniors with reduced autonomy who need several hours of care per day. Most of these facilities receive public financing and are managed by the government. However, within the public system, there are around sixty “private funded” CHSLDs that are subsidized by the government but run by entrepreneurs. (The remaining facilities, private unfunded CHSLDs, are managed independently and receive no public financing.)
On March 31, 2017, Quebec had 317 public CHSLDs, 59 private funded CHSLDs, and 39 private unfunded CHSLDs.(3) The case of private funded CHSLDs is interesting because they receive the same funding as public facilities and are subject to the same conditions: The clientele, accommodation costs, and working conditions are the same. Patients access them through the same regional point of entry and pay the same fee. Private funded facilities are therefore perfectly integrated into the public system, which is how the government presents them.(4) The only difference is the way they are managed, which produces very different results both for users and for the government.
Better Services…
Quality assessment visits of CHSLD living environments, conducted without advance notice by the Department of Health and Social Services,(5) show a very wide gap between the results obtained by public facilities and private funded ones. A previous MEI publication noted this gap in a sample representing half of Quebec’s CHSLDs.(6) A more recent report, obtained following an access to information request, provides an even more complete picture since it covers a little more than 85% of the province’s CHSLDs.
Among the 356 CHSLDs visited between April 1st, 2015 and March 31, 2017, only 17.6% of public facilities (49 out of a total of 279) were considered to be “entirely adequate” by the Department representatives. Some 71% of public facilities were judged to provide an “acceptable” environment, and 11.5% (32 public facilities) were found to have a “worrisome” environment(7) (see Figure 1).
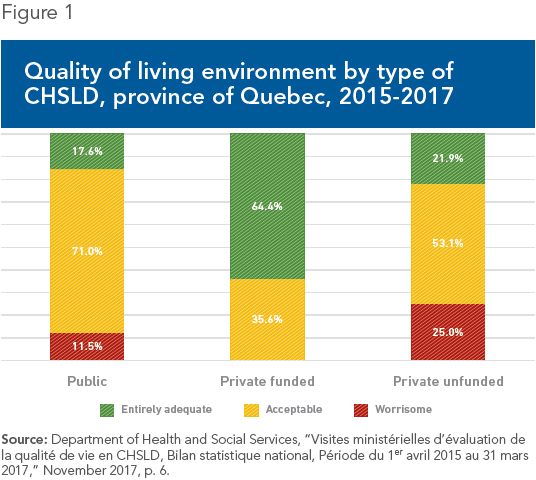
In contrast, the living environments of 64.4% of private funded CHSLDs (29 out of a total of 45) were deemed “entirely adequate,” a proportion nearly four times higher than for public facilities. Not a single private funded CHSLD was considered “worrisome.”
(It is interesting to note the performance of private unfunded CHSLDs, which receive no government funding and must provide the same services with fewer resources. A higher proportion of these facilities were deemed “worrisome” than for public CHSLDs, although a higher proportion of their environments were also considered “entirely adequate” than in public facilities, despite their disadvantage. It is also the case that the gap between the private and public facilities is far smaller than the gap between the public and the private funded facilities.)
… For Less
In addition to providing a better environment for patients, private funded CHSLDs cost the government less, all while succeeding in generating profits for the companies that run them. Indeed, a study carried out a few years ago showed that the total cost per day of attendance was 12% higher in public facilities than in private funded facilities. Looking at operating costs alone (that is, excluding the clinical component), this difference rises to 26%.(8)
The author of the study calculated that entrepreneurial management of the private funded facilities saved the government $30 million a year. He also estimated that there would be a “minimum” of $125 million in additional savings if this method of management were extended across the CHSLD network. In today’s dollars, these amounts are close to $50 million and $200 million respectively. We can only speculate about the sums that could be saved if more efficient methods of management were adopted by even a portion of the hospital network.
A Proven Solution
The superior performance of private funded CHSLDs will not surprise those who are familiar with European health care systems. Over the years, many examples have been noted where, with equal resources, entrepreneurial management has proven superior to public management in terms of the quality of services provided. This has been the case in Germany,(9) Spain,(10) France,(11) and Sweden,(12) among others. The economic literature has also shown that private facilities generally offer better care all while being more efficient.(13)
The performance of our health care systems does not depend only on one variable, and many things can be done to improve them. Greater openness to entrepreneurship within the public systems, all while maintaining universal coverage, nonetheless remains a solution that has proven itself, here and elsewhere. There is no reason not to make more use of it, whether for CHSLDs, for hospitals, or for other components of health care.
References
1. Alain Vadeboncœur, “Le privé sauvera les urgences… vraiment?” L’actualité, August 23, 2019.
2. To be precise, 418 as of March 31, 2019. Committee on Health and Social Services, L’étude des crédits 2019-2020, Ministère de la Santé et des Services sociaux, Réponses aux questions particulières − Opposition officielle, Vol. 3, pp. 13-14.
3. Department of Health and Social Services, “Visites ministérielles d’évaluation de la qualité de vie en CHSLD, Bilan statistique national, Période du 1er avril 2015 au 31 mars 2017,” November 2017, p. 2.
4. Government of Quebec, Santé Montréal, Residential and Long-Term Care Centres (CHSLDS), What is a residential centre? Page consulted September 3, 2019; Committee on Health and Social Services, The living conditions of adults living in residential and long-term care centres – Consultation Document, September 2013, p. 6.
5. Isabelle David, État des connaissances : Qualité du milieu de vie en centre d’hébergement pour les personnes âgées en perte d’autonomie, Institut national d’excellence en santé et en services sociaux, 2018, p. 48.
6. Patrick Déry, “Relying on Entrepreneurs to House and Care for Our Seniors,” Viewpoint, MEI, April 26, 2018.
7. Visits took place in 279 public CHSLDs, 45 private funded CHSLDs, and 32 private unfunded CHSLDs, between April 1st, 2015 and March 31, 2017. Department of Health and Social Services, op. cit., endnote 3.
8. Pierre Fortin, “Examen des coûts d’opération comparatifs des réseaux privé et public en matière de gestion des centres d’accueil et d’hébergement et des centres hospitaliers de soins de longue durée,” Report submitted to the Association des centres hospitaliers et des centres d’accueil privés du Québec, École des sciences de la gestion, Université du Québec à Montréal, November 1996, p. 11.
9. Frederik Cyrus Roeder and Yanick Labrie, “The Private Sector within a Public Health Care System: The German Example,” Economic Note, MEI, February 21, 2012.
10. Yanick Labrie, “The Positive Role of Profit in the Field of Health Care,” Economic Note, MEI, November 6, 2014.
11. Yanick Labrie, For a Universal and Efficient Health Care System: Six Reform Proposals, Research Paper, MEI, March 13, 2014.
12. Patrick Déry and Jasmin Guénette, “Saint Göran: A Competitive Hospital in a Universal System,” Economic Note, MEI, October 17, 2017.
13. See for example Paul H. Jensen, Elizabeth Webster, and Julia Witt, “Hospital type and patient outcomes: An empirical examination using AMI readmission and mortality records,” Health Economics, Vol. 18, 2009, pp. 1440-1460; Karen Eggleston et al., “Hospital ownership and quality of care: What explains the different results in the literature?” Health Economics, Vol. 17, 2008, pp. 1345-1362.