Health Care Entrepreneurship – How to Encourage the Deployment of Telemedicine in Canada

The technologies behind telemedicine are available, and more Canadians could receive remote care, at home or at work, thereby saving themselves trips and avoiding long waits. Unfortunately, our governments are slow to remove obstacles that prevent patients from benefiting from virtual consultations, and doctors from providing this care.
See the study’s graphs at the bottom of the page
 Related Content
Related Content
 |
 |
 |
| Pour un meilleur accès à la télémédecine (La Presse+, September 20, 2019)
Take down the barriers to telemedicine (Montreal Gazette, September 20, 2019) |
Interview (in French) with Patrick Déry (Politiquement incorrect, QUB Radio, September 19, 2019)
Interview (in French) with Patrick Déry (Deux hommes en ondes, FM93, September 20, 2019) |
Interview with Pascale Déry (CTV News Montreal Noon, CFCF-TV, October 6, 2019) |
This Research Paper was prepared by Patrick Déry, Senior Associate Analyst at the MEI.
Highlights
While today’s technology has made it entirely feasible, the use of telemedicine remains limited in Canada and elsewhere, although it is growing, driven mainly by the entrepreneurial sector. Yet the gains that we could reap from greater reliance on remote care are substantial, given the difficulties Canadians have accessing care. Why does the use of virtual consultations remain so marginal today, and how can this be addressed?
Chapter 1 – Where Things Stand
- While all provinces provide certain remote medical services, British Columbia is the only one where video consultations with family doctors are paid for by the government just like any other medical consultation.
- Of the 270 million billable services tallied by the Canadian Institute for Health Information in 2014, only 412,000, or 0.15%, were remote consultations.
- In 2018, only 4% of Canadian family doctors offered their patients the option of a virtual consultation, and only 9% of medical specialists did so. Only 1% of the Canadian population uses telemedicine services.
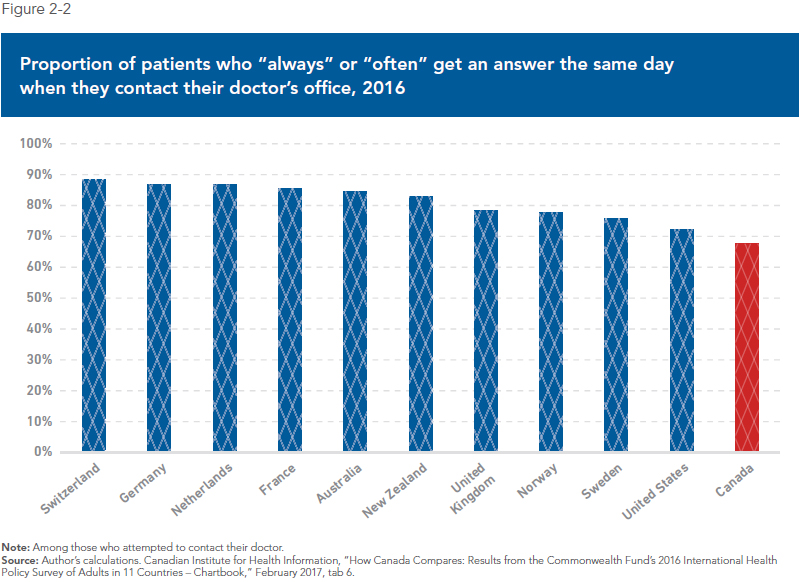
- A 2016 comparison between ten rich countries found that Canadian doctors were the least likely (16%) to offer their patients the option of contacting them by email, versus 86% in Switzerland and 64% in the United States.
- Yet patients appear willing to use technology to access health care. Three-quarters of Canadians say they are interested in using an online portal to access their medical file and consult their doctor, and four in ten are ready to pay for such a service.
- Despite a recent expansion in service provision, the use of virtual consultations also remains limited in Europe, with virtual consultations making up around 2% of primary care visits in Sweden in 2017, for example.
- In the United States, between 2015 and 2018, the proportion of large companies (200+ employees) whose primary group insurance plans covered the use of telemedicine went from slightly more than one-quarter to nearly three-quarters.
- Although the number of virtual visits to doctors by Americans insured under a group plan had risen nearly 20-fold between 2010 and 2016, fewer than 1% of the insured had used that option.
Chapter 2 – Improving Access to Health Care while Reducing Costs
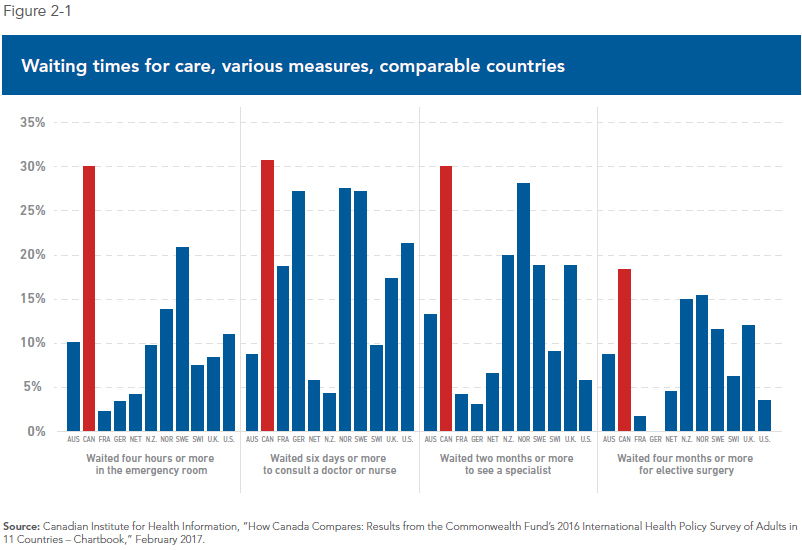
- In a comparison of the health care systems of eleven rich countries, Canada comes in dead last in terms of getting an appointment with a health care professional the same day or the next, in waiting times to see a medical specialist, and in waiting times for elective surgery.
- Canada is also (and by far) the country where people are most likely to spend long hours in a hospital emergency room before getting the treatment they need.
- More than two out of three Canadians (68%) say they have given up on a medical consultation due to various obstacles, such as long waiting times or the inability to see a doctor outside normal office hours.
- The government regards patients as a net expense; it therefore seeks to limit such expenses, notably by restricting and rationing the supply of care. For companies operating in the health care field, patients represent potential income, and they therefore want more of them.
- More than four in ten Canadians thought their latest visit to an ER was for a condition that could have been treated in a clinic; meanwhile, telemedicine companies say that from 50% to 70% of common primary care problems can be dealt with during a virtual visit.
- A number of studies have shown that virtual consultations could lead to cost savings for care providers compared to in-person consultations.
- For employers, offering virtual consultations to their employees could also result in significant savings, as a 2013 study estimated the cost of absenteeism to Canadian employers at close to $17 billion, or 2.4% of the total wage bill.
- There is ample scientific evidence that low-cost telemedicine interventions in primary care are feasible and acceptable to both patients and physicians, and typically result in improved quality of care and cost savings.
Chapter 3 – Obstacles to the Deployment of Telemedicine
- Since the use of telemedicine helps reduce the costs of some treatments, and avoid others altogether, it should in principle lead to efficiency gains for health systems.
- However, if telemedicine allowed the public systems to meet Canadians’ unmet demand for care, this could in theory lead to an increase in government health care spending. At the least, the potential savings could be wiped out by additional demand for care, which would at long last be met.
- Entrepreneurial efforts, which are also being developed outside the public system, may provide a solution by increasing the overall supply of care, all while reducing the pressure on government spending.
- Access to technology is sometimes presented as an obstacle to the development of telemedicine, yet numerous solutions exist and are available on devices that the vast majority of patients and caregivers use every day.
- Regulatory barriers, however, do constitute a real obstacle, as under current rules, a doctor wishing to offer telemedicine consultations in every province will need to possess and renew six or seven provincial licences.
- Relaxing regulations on professional licensing through the mutual recognition of provincial licences, which an overwhelming majority (92%) of doctors favour, could help boost the supply of care and increase access.
- The American example shows that regulatory easing is possible. In early 2019, 24 states had adopted a policy favouring the accelerated issuing of doctors’ licences, while the principle of recognizing nurses’ licences from another state had been adopted by 31 states.
- In addition to licensing-related barriers, most of Canada’s public health care systems limit access to telemedicine by imposing all sorts of conditions that do not exist in the case of entrepreneurial telemedicine.
- Most provincial health care systems restrict the use of telemedicine to patients living in remote areas, or at least give them much higher priority, and require that patients receive care in a place designated or approved for this purpose.
- In several provinces, doctors also have to seek permission or register with the public authorities before they can provide telemedicine-based consultations within the public system.
Chapter 4 – Case Studies: Entrepreneurial Telemedicine and the Ontario Telemedicine Network
- In entrepreneurial telemedicine, patients select their care providers and the times when they receive care. If they are not happy with the services they are getting, they can turn to another provider.
- Companies operating in the entrepreneurial telemedicine sector offer consultations on demand for common health problems by text message, voice, or video, using phones, tablets, or personal computers, at the time and place that suits the patient.
- The definition of “consultation on demand” varies from company to company, with some offering daytime consultations by appointment, others guaranteeing a consultation with a nurse practitioner or a doctor in a matter of minutes, 24 hours a day, seven days a week.
- Most companies providing virtual care focus on common health problems (fever, flu, minor infections, allergies, sexual health, prescription renewals, etc.), which are just the types of ailments for which Canadians go to emergency rooms more often than people in comparable countries.
- The largest of Canada’s provincial telemedicine programs is the Ontario Telemedicine Network (OTN), whose primary service is virtual consultations for patients living in remote areas.
- During the 2017-2018 fiscal year, the OTN facilitated nearly 900,000 remote consultations, which remains a small fraction of the approximately 100 million clinical services delivered each year in the province.
- Still, there is no doubt that the OTN provides substantial benefits for patients and for the public health care system: The programs for virtual consultations between primary care providers and specialists, for instance, have eliminated the need for in-person patient visits in nearly 80% of cases.
- The slow spread of telemedicine within the Ontario public health care system again illustrates the difficulty that bureaucratic systems have in incorporating innovation.
Conclusion – Recommendations for Policy-Makers
The general objective of provincial policy-makers should be to lower the barriers that slow down the development and expansion of telemedicine, which does not entail in itself any additional government spending.
1) Mutual Recognition of Licences to Practise: The need for doctors to hold licences in several provinces is probably the biggest obstacle to the expansion of companies active in the field of telemedicine. It also prevents a better allocation of medical resources in the public systems.
2) Eliminate Professional Barriers: The scope of practice of nurses, nurse practitioners, and pharmacists should be broadened as much as possible; the less that facilities and companies offering telemedicine services will depend on doctors, who are a scarce resource, the more they will be able to expand their services and improve access for patients.
3) Review the Remuneration of Doctors: Canadian doctors receive nearly three-quarters of their remuneration in the form of fee-for-service payments, which does not favour innovation in the practise of medicine.
4) Authorize Mixed Medical Practice: In several European countries, studies have shown that doctors who adopt a mixed practice increase the overall number of hours spent treating patients, without reducing the time devoted to the public system.
5) See the Private Sector as a Partner: Health care systems drawing on the contribution of private companies within universal systems are the norm across the OECD, with impressive results from the perspective of patients and public finances alike. In Canada, companies active in the field of telemedicine have shown that they could provide support to public facilities.
6) Resisting the Temptation to Regulate: The benefits of telemedicine for patients have been amply demonstrated, and its professionals are already governed by codes of ethics and professional orders. Legislators should take a step to the side, and concentrate their action on bringing down the barriers that still remain.
Introduction
The day started badly, like yesterday. Still the same symptoms, but you don’t feel much like spending the morning at a clinic, and an emergency room even less. You open an application on your phone. In a matter of clicks, a doctor’s face appears. After a brief consultation, you are given a prescription, which is delivered to you a little later that day. Without thinking about it too much, you are already back to your daily activities.
Such a scenario was science fiction just a few years ago. Today’s technology has made it feasible, but the use of telemedicine remains limited in Canada, depriving Canadian patients of its benefits. Why is this? And what can be done to remedy the situation? These are the questions that will be addressed in these pages.
What, exactly, is telemedicine? In the broadest sense, it could be defined as the use of any technology that helps health care providers collaborate and deliver remote care to patients.(1)
This can go from a simple doctor-patient phone call to videoconferencing using sophisticated technology, and includes instant messaging and the use of video applications on mobile devices for an exam or a follow-up. This broad definition can also include the telemonitoring of patients with chronic conditions, remote consultations, and the transmission of results or images between health professionals.(2)
This research paper will focus mainly on consultations between patients and caregivers. The latter generally include medical doctors and nurses, although other health professionals can also be involved (psychologists, nutritionists, etc.). There will be discussion of telemedicine, virtual medicine, telehealth, telepractice, telemonitoring, teleassistance, or virtual consultations, depending on the context or the sources, or simply to vary the vocabulary, regardless of which professional is providing care.
The practice of telemedicine, its evolution, and its growth will be examined both within the public health systems and in an entrepreneurial context, the point being to look at what favours its expansion, what slows it, and ultimately, identifying ways of making it accessible to as many patients as possible.
Chapter 1 will sketch a general picture of the adoption of telemedicine and its accessibility in Canada, and provide a brief overview of the situation in comparable countries like Sweden, France, the United Kingdom, and the United States. It will show, among other things, that Canadian doctors are reluctant to adopt new technologies in their practices, even though a large proportion of patients are in favour of them. It will examine how, here and elsewhere, the use of virtual consultations remains marginal, although it is growing, driven mainly by the entrepreneurial sector.
Chapter 2 will describe the gains that Canada could reap from greater reliance on remote medicine. It will first give an overview of the difficulties Canadians have accessing care compared to patients in other industrialized countries. It will survey the benefits for patients in terms of access and reduced waits, and for governments in terms of savings and efficiency. Finally, it will show how the contribution of employers can help make these gains a reality, from the perspective of patients and of the government.
Chapter 3 will look specifically at the main obstacles to the deployment of telemedicine in Canada. It will explain why certain impediments, notably financial and technological issues, are more illustrations of the limits of public systems than actual obstacles to the expansion of telemedicine. It will also show how regulatory barriers, in particular the territorial regulation of professional practice, are a very real obstacle from the perspective of telemedicine companies, but also from the perspective of Canada’s public health care systems, and how to remove this obstacle. Finally, it will note how the rationing of care by government, which imposes all sorts of conditions on providing or receiving remote care, also hinders the deployment of telemedicine.
Chapter 4 will present case studies of different solutions that are offered to patients, in an entrepreneurial context and within the public system. Without carrying out a direct comparison, it will provide an overview of the operations and the services offered by different telemedicine companies to individuals, and even to certain public facilities. It will also give a brief glimpse of the telemedicine of the future. It will then look at the case of the Ontario Telemedicine Network, a publicly funded non-profit organization that generated the most developed network in the country, by examining its benefits for patients, as well as the limits of this model.
In this paper’s conclusion will be found concrete recommendations for our public decision-makers, the common denominator being the abolition of all obstacles to the deployment of telemedicine. These recommendations, whose implementation requires no additional spending by governments, will facilitate the expansion of remote care and favour their wider dissemination by the public health care systems and by companies offering virtual consultations. In the end, they will have the effect of increasing the supply of care and providing better access to patients. They will also have benefits not just for the telemedicine sector, but for Canadian health care as a whole.
Read the Research Paper (in PDF format)
Notes
1. Kerry Waddel, Eilish M. Scallan and Michael G. Wilson, “Understanding the Use and Compensation for Virtual-care Services in Primary Care,” McMaster Health Forum, McMaster University, July 27, 2018, p. 4.
2. World Health Organization, Telemedicine: Opportunities and developments in Member States – Report on the second global survey on eHealth, Global Observatory for eHealth series, Vol. 2, 2010, p. 9; Collège des médecins, Le médecin, la télémédecine et les technologies de l’information et de la communication: Guide d’exercice, February 2015, p. 9.
The graphs (Click to enlarge)
 |
 |
 |
 |
 |
 |